
I am sorry it’s been so long since I’ve sent out an email. I’ve been a bit ‘under the weather’ (I’ll have to look up where that phrase came from). Sue’s been busy doing what Sue does which is just about everything! ::grin::
Disclaimer: Self-treating any eye condition and avoiding or delaying standard care may have serious consequences. Any of these recommendations are not intended to be a substitute for the medical advice given to you by your internist/general practitioner/primary care physician and your retinal specialist.
There’s always frustration when a patient with early AMD is told that they’re not candidates to take the AREDS/AREDS2 supplement. “What do I do?” I get the same question if someone doesn’t have AMD but has a strong family history. What about those who are aging and are concerned about their risk? Those are the same questions asked of eye specialists who have patients in these categories.
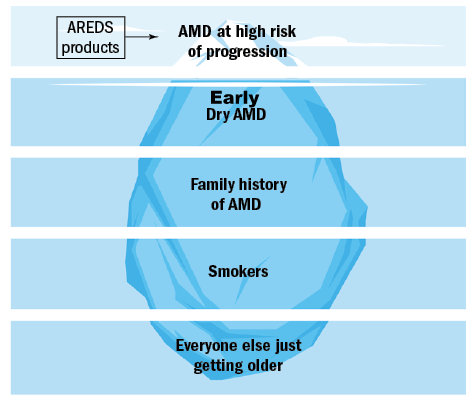
I found an article Beyond the tip of the iceberg – AMD and nutrition written by Dr. Rohit Narayan who is a therapeutic optometrist in England. His October 2018 article reviews some of the more recent studies about how nutrition affects the development and progression of AMD. The AREDS and AREDS2 studies provided the most significant evidence that a specific formulation of vitamins and minerals can reduce the risk of advancing to wet AMD for those who have intermediate AMD or wet AMD in one eye but not the other one. Dr. Narayan considers this group to be at the tip of the iceberg of those who are concerned. He writes, “So, what advice can the busy clinician give to a patient regarding diet and its effect on eye health?”

I’ve taken the illustration of 5 layers of his iceberg and summarized his recommendations for 4 of them. The 5th one (bottom layer) will be coming when he publishes his recommendations in a future article.
Start here: Article: Beyond the tip of the iceberg – AMD and nutrition – Part 1. At the bottom of each page, there’s a link to the next one.

 Click here
Click here
